Researchers have developed a human antibody that targets the opioid fentanyl and its derivatives, blocking the drug’s effects and reversing overdose better than currently available treatments. With clinical trials pending, the novel antibody therapy could be a more effective way of treating life-threatening opioid overdoses.
In the US in 2021, overall deaths from opioid overdose rose above 80,000, with synthetic opioids accounting for most of these deaths. Opioids, whether natural or synthetic, selectively bind to mu-opioid receptors in the brain, causing analgesia, sedation, euphoria and respiratory depression – the lattermost being the primary cause of overdose and death. The main culprits are fentanyl and its structurally related variants.
While fentanyl is about 100 times stronger than morphine and up to 50 times stronger than heroin, carfentanil, a variant, is the most potent opioid used commercially, approximately 10,000 times more potent than morphine. This makes sense considering it was designed to be an elephant tranquilizer. Despite the US Food and Drug Administration (FDA) pulling carfentanil off the market, it’s made its way to the streets, where it’s commonly mixed with heroin and cocaine.
Researchers from the Scripps Research Institute in California have developed a human antibody that binds to carfentanil and other fentanyl variants, reversing the effects of potentially fatal overdose more effectively than currently available treatments.
“We expect this antibody to be a valuable new weapon for fighting the opioid crisis,” said Kim Janda, corresponding author of the study.
Treating a carfentanil overdose is a challenge, given its potency and its ability to bind strongly with mu-opioid receptors. The primary treatment currently is naloxone, which binds to opioid receptors and blocks the drug’s effects. The problem with naloxone is that it’s effects are short-lived and may not be effective against carfentanil overdose. So, the researchers set about finding a solution by developing a human anti-fentanyl antibody.
They vaccinated rats with a molecule they designed to elicit the creation of antibodies against fentanyl and its derivatives. The rats were engineered to produce human antibodies to avoid triggering an unwanted immune response if they were administered to humans. The researchers identified several antibodies that bound strongly with carfentanil and chose the one that was most potent, modified it to be more lightweight and therefore enter the bloodstream quicker, and further altered it so that it would be active in the blood for longer.
The antibody was created in a single-chain variable fragment (scFv) format, a small-sized artificial construct that retains the antigen-binding properties of the corresponding immunoglobulin G (IgG) antibody, the most common type of antibody. scFvs are easier and cheaper to produce than monoclonal antibodies and, while they’re smaller than full-length antibodies, scFVs are used in many of the ways antibodies are.
Testing the optimized scFv antibody, called C10-S66K, in rats, the researchers found that it was powerful at reducing the effects of carfentanil on the brain. When injected, it reversed respiratory depression within 15 minutes after heavy carfentanil exposure. After about 40 minutes, the effect was stronger than that produced by naloxone and continued to increase after two hours, whereas naloxone’s peaked at 30 minutes and swiftly fell off.
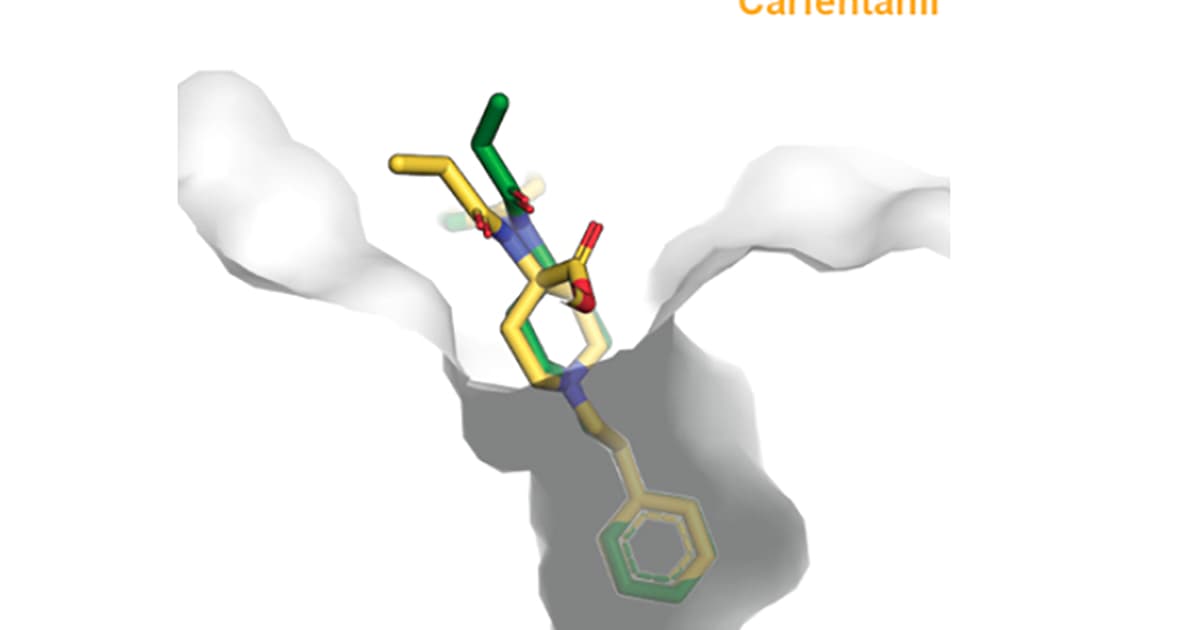
X-ray crystallography used to examine the structure of C10-S66K bound with carfentanil and fentanyl suggested that the antibody would bind well to multiple fentanyl derivatives but shouldn’t interfere with naloxone treatment.
A clinical trial of the C10-S66K antibody is planned for later this month. Meanwhile, the FDA has approved the use of a full-length IgG version of the antibody, CSX-1004, for clinical trials to prevent fentanyl overdose that are also scheduled to commence this month.
The study was published in the journal ACS Chemical Neuroscience.
Source: Scripps Research Institute
Source of Article